Reflections on team development theory in a crisis situation

At the time of writing this post the NHS, the country and indeed the whole world were in the midst of responding to the COVID-19 pandemic and adjusting to the new way in which we need to do our work. Many of us work(ed) in effective established teams with well-oiled group norms and comfortable team roles. In early March 2020 the cards were thrown in the air and we found ourselves having to quickly regroup and respond to the rapidly emerging global pandemic.
I write from the position of working in two organisations: firstly as a jobbing doctor in a large urban GP surgery (practice) and secondly as Chair of a large NHS Clinical Commissioning Group (CCG). This has afforded me the privilege of observing (and being part of) how different teams have responded. I'd like to make some comparisons on this rapid transition and draw in some thoughts on group development theory.
What's been happening?
During the early days of the crisis I observed teams in my clinical practice begin to reform and new leaders emerge playing to their individual strengths and skill sets. Gone were the days of a single strong leader we were used to in our hierarchical health centre. In the chaos all players were in it together and innovation was order of the day. It feels as though we are working in new ways and for the better!
At the CCG we enacted our emergency and business continuity plans, a national command structure was formed and pre-described roles were filled. Here it felt methodical and controlled but almost as though the days of the inclusive and facilitative leadership styles to which we have become accustomed could be a distant memory that will return at some point in the future.
In both organisations the pace of change and transformation have been awe inspiring and something to be proud of. In a short space of time enormous amounts of energy and creativity and a tangible sense of urgency have resulted in more innovative changes in health care provision than have been achieved in the past decade. Despite these amazing efforts there is still much to be done but in both settings but I can't help ask myself if this positive energy is at risk of burning itself out? What might be happening? Let's look at some theory.
Group Development Models and Virtual Working
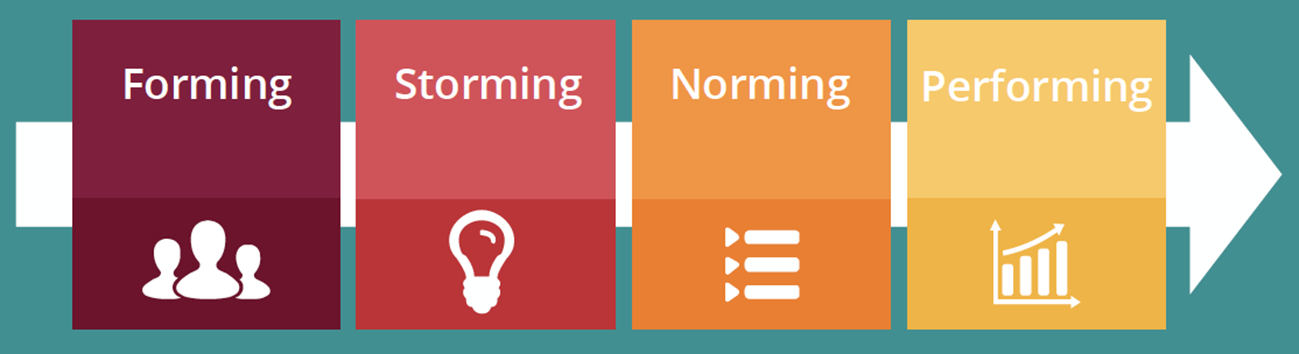
Many leaders (and indeed lay people) will be familiar with Bruce Tuckman's famous Team Development Model:
Forming >> Storming >> Norming >> Performing
In summary, Tuckman describes groups of people with defined skills coming together in the pursuit of a common goal with direction from a leader. Processes are often ignored but the leader directs the team. In the second "storming" phase team members vie for position as they attempt to establish themselves, cliques form and power games play out. Clarity of purpose increases and leaders coach. Following this stage the group begins to establish its "norms": agreement and consensus on roles, responsibilities and processes. Finally the team begins to effectively perform to a shared vision.
So what, if anything, is different now?
"Our teams are already formed and established!" But are they really?
Suddenly we are responding to a crisis none of us have ever encountered before. To exacerbate matters members of our teams have been redeployed to new roles and unfamiliar staff are supporting the efforts of established teams. The nature of the pandemic means many staff are now working from home and we now find ourselves working in a new territory: virtual teams.
What's a virtual team?
A virtual team isn't just working from home. By definition a virtual team is a group of people working in pursuit of a common goal, but separated by location, time or culture/organisation.
So what?
Our teams are now disrupted by a new unfamiliar scenario, with new team members and the challenge of working in a virtual way. Our familiar teams are now having to redevelop. But is this new team development following Tuckman's model? I believe not.
In both organisations the teams performed. They rapidly rallied together in a common pursuit and achieved what was needed. However, the complication of working in a virtual manner (separated by place) has caused both organisations to ask questions and look at the way they work through a new lens.
- How do we make decisions now?
- What is the new norm for communicating? Email? Text? Video conference?
- How do we diffuse group conflict when people aren't together?
- How do we meet to discuss things? What is the etiquette for a virtual meeting on Zoom?
- How do we know who is really doing what?
- Do we really need to bring all of our patients in to the clinic? Why weren't we calling people up or doing video consultations years ago?
The complication of working in a virtual manner has caused organisations to look at the way they work through a new lens.
So, both teams started by performing then realised that what was needed was a new phase of "norming": establishing a new set of rules and procedures to ensure the slick functioning of the group, in the context of doing this in a virtual setting separated by location (from our homes), by time (those with kids and other commitments aren't always available when others are) and by culture (working as with those from other health and care organisations are part of a system).
Thought is going into communication methods and technology. The tech is an enabler and not a solution in its own right. Attention is being paid to the differences between synchronous and asynchronous communications methods and the appropriateness of different methods.

Taking Group Development to the Next Stage
In establishing some new norms, the teams in both organisations are reflecting on what new roles were needed for effective group performance. Who is really best to lead on a set work stream? What skills sets are there within the groups and what strengths could be played to help achieve the goals? Some people might now find themselves doing something very different to their normal role. The essence is that it might be the same role but, but it is still an important role. This is phase is almost akin "forming" a team, with a subtle blend of storming minus the team conflict.
It is important we don't miss the softer team interactions which truly bond teams
In this new "forming" stage in the virtual world it is important we don't miss the softer team interactions which truly bond teams: the coffee room chats, the corridor conversations, the team lunches, the opportunities for professional growth and checking-in with or showing an interest in our colleagues (and in many cases our professional friends). These are more challenging in a virtual environment but not impossible.
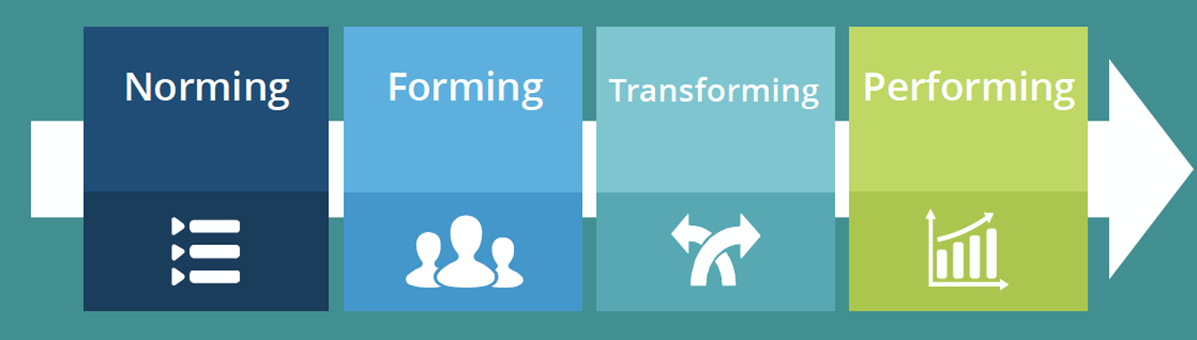
Moving on from the norming and forming, the teams will begin to reach a "transforming" stage where the new team norms are practiced and refined in the context of new roles and team members adjust to their new roles. Leadership in this phase will be facilitative and transformative.
Eventually these virtual teams will overcome the challenges of working in a new virtual context and become high performing virtual teams. In many respects both teams have already proved they are high performing, but are now adjusting to a new "normal" world in which we find ourselves.
Future Opportunities
I find the nature of our GP surgery moving from a very transactional leadership model to a transformative way of working, in contrast to the CCGs transformational leadership becoming more transactional in its command-and-control model, a fascinating contrast. Both organisations seemingly moving in different directions have followed the same team development stages. I'm sure as both organisations develop a rhythm for their new manner of working a happy medium between transformative and transactional leadership will emerge.
None us can be certain about what the future holds, but it is almost certain that the way we work will be transformed forever. Many of us are longing to get back in to our offices, avoid the "social distance-dance" of keeping 2 metres away from the nearest human being and to chat with trusted colleagues over a cup of tea. I sincerely hope that all team members can capture the journeys they took and reflect on the different ways their teams developed to achieve outstanding transformation and apply this to new visionary ways of working in the future. From every crisis comes an opportunity.
Author | Dr Terry Hudsen

Dr Terry Hudsen is a UK-based General Practitioner with a portfolio career that spans clinical practice, system leadership and cross-sector collaboration.
In addition to his clinical work, Terry previously served as Chairman of NHS Sheffield Clinical Commissioning Group (CCG), leading strategic commissioning and system redesign, as well as leading the complex organisational change and transition to Integrated Care Boards. During this he led the establishment of joint commissioning arrangements between the NHS and local authorities and played a part in shaping national policy on maintaining joint health and care commissioning arrangements for local decision-making in place-based health and care systems.
Following the dissolution of CCGs in 2022, he became lead for Population Health and System Development in South Yorkshire’s Integrated Care System, before leaving the NHS to establish an independent consultancy supporting NHS providers, local authorities and VCSE organisations with their capabilities for developing collaborative leadership, strategy and tackling wicked problems.
In 2023, he became Independent Chair of the Bradford Safeguarding Adults Board, where he leads a statutory partnership which comprises partners from health, social care, local government, police, and the voluntary, community and social enterprise (VCSE) sector, focussing on preventing and responding to harm, neglect and exploitation of vulnerable adults.
Alongside these roles, Terry is Clinical Lead for Primary Care and Neighbourhood Engagement and Support within NHS England’s mental health portfolio in the North East and Yorkshire, helping to drive transformation and strengthen collaboration between providers of health and care at local level.
In addition to his medical qualifications from the University of Sheffield, Terry is a proud alumnus of The Open University Business School, where he earned an MBA with distinction in Leadership Practice. He is a Chartered Manager and a Fellow of the Chartered Management Institute. He is particularly interested in leadership across organisational boundaries, with his MBA dissertation focussing on collaboration between the NHS and VCSE sector.
In all his roles he emphasises the power of partnership, culture and shared learning in creating sustainable change. Passionate about building a culture of curiosity and shared purpose across public services, he writes and speaks about adaptive leadership, collaboration and innovation in complex systems. His work aims to inspire leaders and practitioners to think differently, work collectively, and create meaningful impact in the communities they work.
Article previously published on LinkedIn.
December 2025
Would you like to contribute an article towards our Professional Knowledge Bank? Find out more.

Stay in touch


Explore

Undergraduate
Postgraduate
Policy
-
Follow us on Social media
-


